Maternal hypertension and cardiovascular medications dysregulate placental arterial tone
Maternal hypertension and cardiovascular medications dysregulate placental arterial tone
Tropea, T.; Cottrell, E. C.; Wallworth, R.; Khalil, N.; Johnstone, E.; Myers, J.; Brownbill, P.
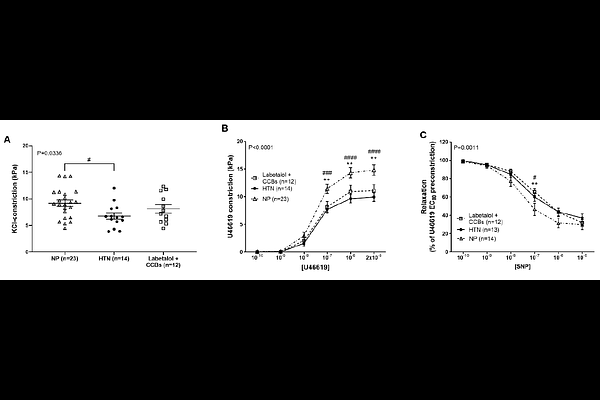
AbstractCardiovascular medications prescribed to pregnant women include Ca2+ channel blockers (CCBs; amlodipine, nifedipine), - (doxazosin) and {beta}- (labetalol, bisoprolol, nebivolol) adrenergic receptor antagonists, and -adrenergic receptor agonists (methyldopa). These vasoactive drugs enter the fetal circulation, with unknown effects on the fetoplacental vasculature. This study investigates whether cardiovascular medications alter human fetoplacental vascular tone and placental perfusion. Chorionic plate arteries (CPAs) were obtained from placentas of normotensive women (N=28), women with unmedicated hypertension (N=14), and those chronically medicated (N=61) with amlodipine, nifedipine, labetalol or bisoprolol, or CCB-labetalol combinations. Using wire myography, ex vivo concentration-dependent effects of amlodipine, nifedipine, labetalol, methyldopa, doxazosin, bisoprolol and nebivolol were tested in pre-constricted CPAs from normotensive pregnant women. Vascular reactivity following chronic hypertension and/or medication exposure was assessed by vasoconstriction to high potassium physiological solution (KPSS) and U46619, and by relaxation to sodium nitroprusside (SNP). In CPAs from normotensive women, acute exposure to amlodipine, nifedipine, doxazosin and nebivolol promoted vasorelaxation (P<0.05), while labetalol, methyldopa (P<0.05) and bisoprolol (P<0.001) increased vasoconstriction compared to their controls. Chronic hypertension and labetalol-treatment reduced vasoconstriction to KPSS (P<0.05). Chronic hypertension and bisoprolol-treatment attenuated vascular responses to U46619 and SNP (P<0.01 and P<0.01, respectively), compared to normal pregnancy. Maternal hypertension impairs placental vascular function, and cardiovascular medications may further dysregulate fetoplacental vascular reactivity. Further research is warranted to evaluate the relative safety of cardiovascular medications in pregnancy, as their distinct effects on fetoplacental vascular function may impact maternal and fetal outcomes. Mechanistic studies alongside clinical correlations are essential to guide evidence-based prescribing.